Hiatal Hernia Surgery in Houston
Dr. Elias Darido has performed over 1,000 hiatal hernia repair and anti-reflux procedures and specializes exclusively in acid reflux and hiatal hernia management at Houston Heartburn and Reflux Center. He is fellowship-trained in acid reflux and hiatal hernia surgery and has been recognized as a leading hiatal hernia surgery expert in the greater Houston area.
What Is a Hiatal Hernia?
A hiatal hernia develops when part of the stomach pushes upward through the hiatus, the natural opening in the diaphragm (breathing muscle) through which the esophagus passes from the chest into the abdomen. When this opening weakens or enlarges, the upper portion of the stomach can slide or push through it into the chest cavity.
Hiatal hernias are one of the most common anatomic findings in patients with chronic acid reflux. They weaken the anti-reflux barrier (the complex structure that prevents stomach contents from flowing back into the esophagus) and are a major contributor to gastroesophageal reflux disease (GERD). However, not all hiatal hernias are associated with reflux, and the type of hiatal hernia determines both the symptoms and the treatment approach.
At Houston Heartburn, Dr. Darido performs hiatal hernia repair using a minimally invasive laparoscopic or robotic-assisted approach, which means smaller incisions, less pain, and a faster recovery compared to traditional open surgery.
Key facts at a glance:
- Procedure time: Typically 60-90 minutes (when combined with fundoplication)
- Hospital stay: Usually same-day or one overnight stay
- Return to work: Most patients return within 1 week
- Return to full activity: 4-6 weeks
- Long-term success rate: At Houston Heartburn and Reflux Center, our hiatal hernia recurrence rate for sliding hernias repaired with Nissen fundoplication is less than 1%, with a long-term durability exceeding 99%
How Does a Hiatal Hernia Cause Acid Reflux?
The root cause of GERD is a weak or dysfunctional anti-reflux barrier. The anti-reflux barrier is a complex anatomical and physiological structure that prevents stomach content from escaping up into the esophagus. The most commonly known component of the anti-reflux barrier is the lower esophageal sphincter, a muscular ring that acts as a one-way valve between your esophagus and stomach. When this valve does not close properly, stomach acid flows back into the esophagus, causing heartburn, regurgitation, and over time, potential damage to the esophageal lining.
The remaining anatomical components of the anti-reflux barrier are:
Right and left crura of the diaphragm: these are the muscular edges of the opening in the breathing muscle that support the lower esophageal sphincter.
Phrenoesophageal membrane: the fibrous tissue that connects the lower esophageal sphincter to the crura.
Angle of His: the sharp angulation between esophagus and stomach creates a flap that closes the bottom of the esophagus in response to increased stomach pressure.
When a hiatal hernia develops, these components are disrupted. The stomach pushes through the hiatal opening, the crural muscles weaken and spread apart, the phrenoesophageal membrane stretches, and the Angle of His is obliterated. The result is a dysfunctional anti-reflux barrier that allows acid, bile, and digestive enzymes to flow freely back into the esophagus.
This is why medication alone cannot fix a hiatal hernia. Proton pump inhibitors (PPIs) reduce acid production, but they do not restore the structural defect. A hiatal hernia is an anatomical problem that requires surgical correction.
It is very important for Dr Darido that you understand the exact relationship between hiatal hernia, in particular sliding hiatal hernia, and acid reflux. There is a temporal, bi-directional, relationship between acid reflux and hiatal hernia that most patients and physicians fail to understand. When doctors perform tests such as endoscopy or imaging, they may find a sliding hiatal hernia in someone who has reflux symptoms. Because they are present at the same time, it can appear that a hiatal hernia causes reflux. But this does not always explain how the problem started.
The initial instigator of acid reflux is a weak or unstable lower esophagus sphincter. The valve can open unexpectedly through events called transient lower esophagus sphincter relaxation, TLESRs. Early in this stage, reflux episodes happen occasionally, symptoms are mild, and no hiatal hernia is present yet. Over time, frequent reflux episodes result in increased inflammation at the junction between esophagus and stomach. This weakens the fibrous tissue (phrenoesophageal membrane) that holds the anti-reflux barrier structure together, and causes the esophagus to retract upwards towards the chest.
As these structures weaken and with progressive esophagus upward retraction, the top of the stomach slowly slides through the hiatus into the chest. This is how a sliding hiatal hernia forms. Once the hiatal hernia develops, reflux becomes much easier. From this perspective, acid reflux causes a sliding hiatal hernia to develop and a sliding hiatal hernia facilitates more acid reflux to occur.
Small sliding hiatal hernias are extremely common especially as people get older. These hernias are caused by wear and tear to the gastroesophageal junction as opposed to acid reflux. Most of the time, these hernias are asymptomatic.
Types of Hiatal Hernias
There are four types of hiatal hernias. Understanding the differences is critical because the type determines the symptoms you experience, the risks you face, and the surgical approach required.
Type 1: Sliding Hiatal Hernia
The most common type, accounting for approximately 95% of all hiatal hernias. In a sliding hiatal hernia, the gastroesophageal junction (where the esophagus meets the stomach) slides upward through the hiatus. Most GERD patients have a sliding hiatal hernia, but most people with a sliding hiatal hernia don’t have GERD. If left unrepaired, a symptomatic sliding hiatal hernia tends to get bigger with time, resulting in a progressively weaker anti-reflux barrier and worsening acid reflux symptoms.

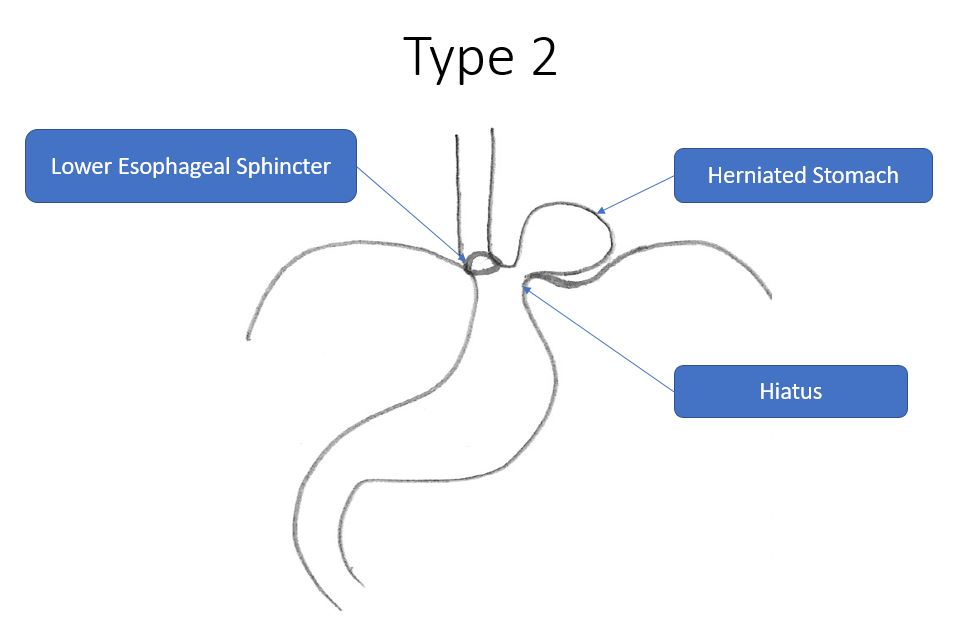
Type 2: Paraesophageal Hernia
In a Type 2 hernia, the gastroesophageal junction stays in its normal position, but part of the stomach herniates upward alongside the esophagus through a weakened hiatus. These hernias are typically not associated with GERD. Contributing factors include age, collagen synthesis genetic abnormalities, and abnormally curved spine. Most patients have minimal symptoms, but some report difficulty swallowing, pain, heartburn, nausea, vomiting, and shortness of breath. Ulcers may develop in the herniated stomach leading to blood loss and anemia.
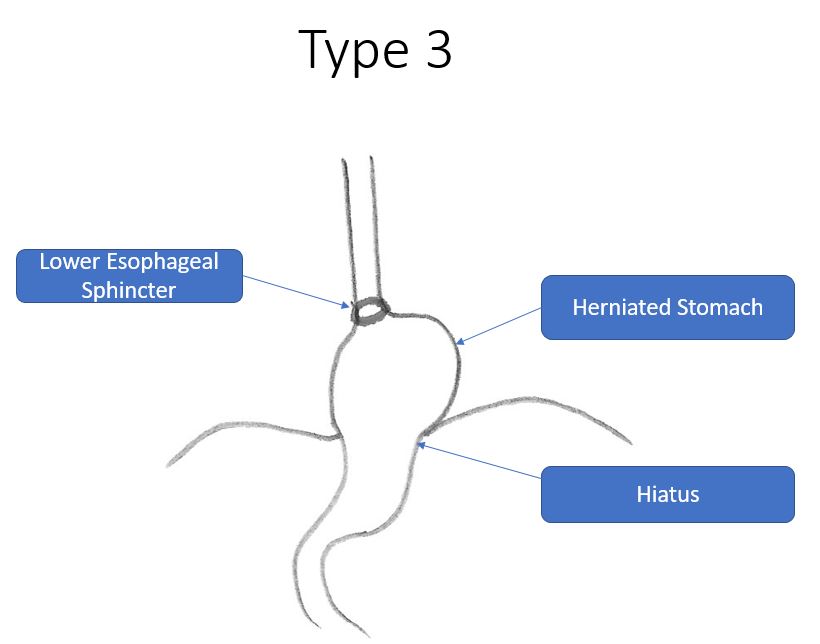
Type 3: Combined Hernia
A Type 3 hernia combines features of both Type 1 and Type 2. Both the gastroesophageal junction and the gastric fundus and body herniate into the chest. This type can be associated with both reflux symptoms and mechanical symptoms like pain, bloating, and shortness of breath.
Type 4: Complex Paraesophageal Hernia
Similar to Type 3 but with additional organs, such as the colon or spleen, herniating into the chest alongside the stomach. This is the most complex type and carries the highest risk of complications.
The Gastric Volvulus Emergency
Both Type 3 and Type 4 hiatal hernias are associated with gastric volvulus. Gastric volvulus occurs when the stomach twists on itself in the chest leading to obstruction and decreased gastric blood perfusion. Patients present with acute onset pain and bloating without being able to vomit. This condition is considered a surgical emergency requiring immediate repair to prevent gastric tissue necrosis, sepsis, and possible death.
Sliding vs. Paraesophageal Hiatal Hernia: Key Differences
| Sliding (Type 1) | Paraesophageal (Types 2-4) | |
|---|---|---|
| Frequency | ~95% of all hiatal hernias | ~5% of all hiatal hernias |
| Associated with GERD? | Yes: strongly associated | Typically no |
| Primary symptoms | Heartburn, regurgitation, chronic cough, hoarseness | Difficulty swallowing, chest pain, bloating, shortness of breath, nausea, anemia |
| Emergency risk | Low (progressive worsening of GERD) | Higher: risk of gastric volvulus and strangulation |
| Surgical approach | Hiatal hernia repair + fundoplication (Nissen or Toupet) | Hiatal hernia repair +/- fundoplication; may include stomach anchoring |
| What happens if untreated? | Hernia grows larger, GERD worsens, risk of Barrett’s esophagus | Risk of volvulus, strangulation, ulcers, anemia, emergency surgery |
| Recurrence rate | Less than 1% at Houston Heartburn (with Nissen) | Up to 50% at 5 years nationally for Types 2-4 |
At Houston Heartburn and Reflux Center, we mainly treat Type 1 or sliding hiatal hernias for GERD management. The pathophysiology of Type 1 hiatal hernias is closely linked to GERD and is dramatically different from that of Types 2, 3, and 4. For this reason, the surgical approach must be tailored to the hernia type: not every patient should receive the same operation.
Who Is a Candidate for Hiatal Hernia Repair?
Not every patient with a hiatal hernia needs surgery. Hiatal hernia repair is typically recommended when:
- You have a sliding hiatal hernia with GERD that no longer responds to medication. You have been taking proton pump inhibitors (PPIs) like omeprazole or pantoprazole for years and your symptoms are breaking through, or your reflux has worsened despite medication.
- You want to stop taking PPIs long-term. There is growing concern about the long-term side effects of PPIs, including bone density loss, kidney issues, and nutrient malabsorption. Many patients seek surgery specifically to eliminate their dependence on daily medication.
- You have volume reflux or regurgitation. PPIs reduce acid production but do not stop the physical backflow of stomach contents. If you experience regurgitation (food or liquid coming back up), medication alone will not solve this.
- You have extra-esophageal reflux symptoms. Chronic cough, hoarseness, throat clearing, asthma-like symptoms, or dental erosion caused by reflux often respond poorly to medication but improve significantly after hiatal hernia repair with fundoplication.
- You have a symptomatic paraesophageal hernia. Symptoms include difficulty swallowing, chest pain, shortness of breath, nausea, vomiting, and anemia from ulcers. Large paraesophageal hernias carry a risk of gastric volvulus and strangulation and should be repaired.
- Objective testing confirms a structural defect. At Houston Heartburn and Reflux Center, we require objective diagnostic confirmation before recommending surgery. This includes upper endoscopy, and in certain cases, ambulatory pH testing and esophageal manometry.
Who is NOT a candidate?
- Patients whose symptoms are controlled well on medication and who are comfortable continuing medication long-term
- Patients with asymptomatic sliding hiatal hernias and no evidence of GERD. In the absence of acid reflux, there is no indication to repair an asymptomatic sliding hiatal hernia as it poses no risk of complications
- Patients with certain esophageal motility disorders (such as achalasia) that require different surgical approaches
- Patients with uncontrolled medical conditions that make general anesthesia high-risk
This is why proper pre-operative workup matters. Dr. Darido has seen many patients referred from other practices where surgery was recommended without adequate testing. At Houston Heartburn and Reflux Center, every surgical candidate completes a comprehensive evaluation before any procedure is discussed.
The Pre-Operative Workup: What to Expect
A thorough evaluation for proper patient selection is what separates a successful outcome from a failed one. At Houston Heartburn and Reflux Center, the standard pre-surgical workup includes:
- Upper Endoscopy (EGD) A scope is passed through the mouth to visually inspect the esophagus, stomach, and duodenum. This identifies the presence and size of a hiatal hernia, any esophageal damage (such as Barrett’s esophagus, a precancerous condition, or esophagitis), and rules out other conditions.
- Esophageal Manometry A thin catheter is placed through the nose into the esophagus to measure the strength and coordination of esophageal contractions as well as lower esophageal sphincter pressure. This test determines whether a full Nissen wrap or a partial Toupet wrap is more appropriate for you. If anti-reflux surgery is decided, this test is performed.
- pH Testing (pH Bravo capsule) A 96-hour acid monitoring study that measures how much acid is actually refluxing into your esophagus. This provides objective proof of GERD and helps predict how well surgery will work for you.
- Barium Swallow (Upper GI Series) An X-ray study where you drink a contrast liquid while images are taken. This shows the size and position of a hiatal hernia and evaluates the anatomy of the esophagus and stomach.
What Happens During Surgery: Step by Step
Before the procedure
You will stop all medications that thin the blood one week prior to surgery. Nothing to eat or drink after midnight the night before. Surgery is performed under general anesthesia.
During the procedure
5 small incisions are made in the upper abdomen (the largest is typically 12mm). All incisions are infiltrated with long-acting numbing medications to decrease pain after surgery.
Dr. Darido uses laparoscopic or robotic-assisted instruments with a high-definition camera.
- The hernia sac is completely dissected and removed. Complete sac removal is critical to reducing recurrence.
- The stomach is returned to its proper position below the diaphragm.
- The distal esophagus is mobilized to ensure adequate length below the diaphragm. This is important because if the esophagus is too short, it can pull the repair back into the chest, leading to recurrence.
- The hiatal opening is closed (crural repair). The right and left crural muscles are approximated with pledgeted sutures under no tension. The closure is carefully calibrated: not too tight (which would cause difficulty swallowing) and not too loose (which would allow recurrence).
- If indicated, biologic mesh reinforcement is placed. At Houston Heartburn, mesh is not used routinely. It is reserved for cases where the right crus is significantly weakened, thinned, or has lost muscle mass. Only absorbable biologic mesh is used, it is never placed in direct contact with the esophagus (at least 5mm gap), and it is fixated with biologic glue to prevent displacement.
- For Type 1 (sliding) hiatal hernias with GERD, a Nissen fundoplication (360-degree wrap) or Toupet fundoplication (270-degree partial wrap) is performed to restore the anti-reflux barrier. The choice depends on esophageal motility testing results and intraoperative findings. For Types 2-4 without GERD, fundoplication may not be necessary and an anchoring procedure may be more appropriate.
The entire procedure typically takes 60-90 minutes.
Immediately after
Most patients go home the same day or after one overnight observation. You will start on a liquid diet and gradually advance to soft foods over 2-4 weeks. Pain is typically managed with over-the-counter medications within a few days.
Hiatal Hernia Repair: With or Without Fundoplication?
One of the most important decisions in hiatal hernia surgery is whether to add a fundoplication. The answer depends entirely on the type of hernia and the presence of GERD.
| Repair + Fundoplication | Repair Without Fundoplication | |
|---|---|---|
| Best for | Type 1 (sliding) hiatal hernias with GERD | Types 2-4 (paraesophageal) without GERD |
| Acid reflux control | Excellent: restores the complete anti-reflux barrier | Does not address reflux (not needed if GERD is absent) |
| Dysphagia risk | Low (0% at Houston Heartburn) | Low |
| Recurrence rate | Less than 1% (Houston Heartburn) | Higher for paraesophageal hernias (up to 50% nationally at 5 years) |
| Key principle | GERD requires restoration of anti-reflux barrier; hiatal hernia repair alone is insufficient | Adding fundoplication when GERD is absent adds minimal risk, and may help anchor the stomach below the diaphragm |
At Houston Heartburn and Reflux Center, a sliding hiatal hernia repair is always associated with a Nissen fundoplication to restore the anti-reflux barrier, and control GERD. However, for Types 2, 3, and 4 paraesophageal hernias that are not associated with GERD, adding a fundoplication may be unnecessary.
Hiatal Hernia Repair vs. Long-Term PPI Medication
Many patients with hiatal hernias are told to manage their symptoms with proton pump inhibitors (PPIs) indefinitely. While PPIs are effective at reducing acid production, they do not address the structural cause of the problem.
| Hiatal Hernia Repair + Fundoplication | PPI Medication (Long-Term) | |
|---|---|---|
| Addresses structural defect? | Yes: restores anatomy and anti-reflux barrier | No: reduces acid but hernia remains |
| Stops all reflux? | Yes: stops acid, bile, and volume reflux | No: reduces acid only; bile and volume reflux persist |
| Duration | One-time procedure with long-term results | Must be taken daily, indefinitely |
| Long-term side effects | Surgical risks (less than 1% complication rate) | Bone density loss, kidney issues, nutrient malabsorption, increased infection risk |
| Best for | Patients with structural defect, failed medical therapy, or who want to eliminate medication | Mild GERD without significant hernia; patients who are not surgical candidates |
When a competent acid reflux surgeon is available to offer high quality hiatal hernia repair and Nissen fundoplication for the right patient, Dr Darido recommends early surgical intervention. Reliable early control of GERD reduces structural damage to the anti-reflux. Consequently, sutures are more likely to hold, leading to a more durable repair.
Download a case study presentation on Hiatal Hernia Repair by Dr. Elias Darido
Recovery After Hiatal Hernia Repair
The First 2 Weeks
- Diet: Clear liquids for the first day, progressing to full liquids like yogurt, Jello, and strained soups. Protein shakes are recommended. You can drink coffee or tea.
- Activity: Light walking is encouraged immediately. Avoid lifting anything over 10-15 pounds.
- Common experiences: Mild difficulty swallowing (expected and temporary), bloating, and some shoulder pain from the gas used during laparoscopic surgery.
- Work: Most patients with desk jobs return to work within 5-7 days.
Weeks 2-4
Diet: Gradual transition to soft, pureed foods. Use a blender to puree ground meat, tuna, and chicken. Avoid bread, pasta, rice, and raw vegetables during this phase. These can be difficult to swallow while the surgical area is still swollen.
- Activity: Gradual return to exercise. Walking, light jogging, and upper body movement can resume.
- Swallowing: Any post-operative dysphagia (difficulty swallowing) typically resolves within 2-4 weeks after surgery as swelling decreases and the repair settles.
Weeks 4-6
- Diet: Normal diet. Most patients are eating comfortably by week 4-6, though portion sizes may be smaller initially.
- Activity: Avoid heavy weight lifting and core-intensive exercise till 6 weeks after surgery.
6 Weeks and Beyond
Most patients are fully recovered and eating a normal diet. All patients who had GERD stop all reflux medications permanently. Follow-up appointment with Dr. Darido to evaluate outcomes.
What about long-term side effects?
Recurrence: The risk of hernia recurrence depends on the type. For sliding hiatal hernias repaired with Nissen fundoplication at Houston Heartburn, the recurrence rate is less than 1%. For paraesophageal hernias, national recurrence rates approach 50% at 5 years, which is why surgical expertise and technique matter significantly.
Success Rates and Long-Term Outcomes
Hiatal hernia repair combined with Nissen fundoplication has been studied extensively. The research consistently shows:
- 85-95% of patients report significant improvement or complete resolution of heartburn and regurgitation symptoms. At Houston Heartburn and Reflux Center, our success rate exceeds 99%.
- 80-90% of patients are able to stop taking PPIs entirely after surgery. At Houston Heartburn and Reflux Center, all patients stop PPIs after surgery.
- Patient satisfaction rates are consistently high in long-term follow-up studies. At Houston Heartburn and Reflux Center, we have performed more than 1,000 hiatal hernia repair and anti-reflux procedures.
- Durability: The procedure maintains its effectiveness in the majority of patients at 10 and 20-year follow-up. At Houston Heartburn and Reflux Center, our long-term durability is more than 99%.
The strongest predictor of a good outcome is proper patient selection, thorough pre-operative testing, correct identification of hernia type, and flawless surgical technique. In expert hands, patients with objectively confirmed GERD, a clear anatomic defect, and symptom relief on PPIs tend to have the best surgical outcomes.
Hiatal Hernia Repair Cost and Insurance
Hiatal hernia repair is a medically necessary procedure and is covered by most insurance plans. Coverage typically requires documentation of:
- Failed or inadequate response to medical therapy (usually 3-6 months of PPI use)
- Objective evidence of GERD (pH testing, endoscopy findings)
- Presence of a hiatal hernia or anatomic defect
At Houston Heartburn and Reflux Center, our team handles insurance verification and prior authorization. We work with most major insurance carriers. If you are unsure about your coverage, contact our office for a benefits check before your first appointment.
For self-pay patients, we offer transparent pricing and payment plan options. Please call (832) 945-8717 to discuss self-pay rates.
Why Choose Houston Heartburn for Hiatal Hernia Repair
Specialized expertise. Unlike general surgeons who perform hiatal hernia repair occasionally, Dr. Darido focuses exclusively on foregut surgery: acid reflux, hiatal hernias, and esophageal conditions. This level of specialization translates to refined technique, fewer complications, and better outcomes.
Comprehensive diagnostic workup. Every patient undergoes objective testing before surgery is recommended. We do not operate on patients who will not benefit from surgery. This commitment to proper evaluation is why our outcomes consistently exceed national averages.
Tailored surgical approach. Dr. Darido does not apply a one-size-fits-all approach. The type of hernia, the presence or absence of GERD, esophageal motility testing, and intraoperative findings all determine the specific surgical technique. Type 1 hernias with GERD receive fundoplication. Types 2-4 without GERD may receive an anchoring procedure instead.
Revision surgery experience. Dr. Darido regularly treats patients whose previous hiatal hernia repair or fundoplication (performed elsewhere) has failed. This experience with complex, redo cases gives him a deep understanding of what makes a repair succeed long-term and what causes them to fail.
High patient satisfaction.
Frequently Asked Questions
What is a hiatal hernia?
A hiatal hernia occurs when the upper part of the stomach pushes upward through the diaphragm into the chest. This displacement weakens the anti-reflux barrier and commonly contributes to GERD.
How many types of hiatal hernias are there?
There are two main categories: sliding (Type 1), which accounts for 95% of cases and is strongly associated with GERD, and paraesophageal (Types 2-4), where the stomach herniates alongside the esophagus and carries a risk of gastric volvulus.
Does a hiatal hernia need surgery?
Not always. Asymptomatic sliding hiatal hernias without GERD do not require repair. Surgery is recommended for symptomatic sliding hernias with GERD that no longer responds to medication, and for paraesophageal hernias due to the risk of volvulus and strangulation.
What happens if you do not repair a hiatal hernia?
For sliding hiatal hernias with GERD: the hernia grows larger over time, the crural muscles weaken further, and GERD worsens. For paraesophageal hernias: the risk of gastric volvulus (stomach twisting) and strangulation increases, which is a life-threatening surgical emergency.
Is hiatal hernia repair the same as Nissen fundoplication?
No. Hiatal hernia repair addresses the structural defect by closing the widened hiatal opening. Nissen fundoplication restores the anti-reflux valve by wrapping the stomach around the esophagus. For Type 1 hernias with GERD, both are performed together. Hiatal hernia repair alone is not sufficient to control acid reflux.
How is hiatal hernia repair done?
Repair is performed laparoscopically or robotically through 5 small incisions. The stomach is returned to the abdomen, the hiatus is tightened with pledgeted sutures, and if GERD is present, the anti-reflux valve is restored with a Nissen or Toupet fundoplication.
How safe is hiatal hernia repair?
In expert hands, hiatal hernia repair is a very safe procedure with a complication rate of less than 1%.
Does Dr. Darido use mesh for hiatal hernia repair?
Not routinely. Pledgeted sutures are effective when the crural muscles are strong. Absorbable biologic mesh is reserved for cases where the right crus is significantly weakened. The mesh is never placed in direct contact with the esophagus.
Can I eat normally after hiatal hernia repair?
Yes. After a 4-6 week recovery diet (liquids to soft foods to regular foods), most patients eat a completely normal diet.
How long does hiatal hernia surgery take?
Typically 60-90 minutes. Including pre-operative preparation and recovery room time, plan for approximately 3-4 hours total at the hospital.
What is the recurrence rate for hiatal hernia repair?
At Houston Heartburn, the recurrence rate for sliding hiatal hernias repaired with Nissen fundoplication is less than 1%. Nationally, paraesophageal hernia recurrence approaches 50% at 5 years.
Does insurance cover hiatal hernia repair?
Yes. Insurance plans routinely cover this medically necessary surgery.
Who is the best hiatal hernia surgeon in Houston?
The best surgeons are those who specialize in GERD and hiatal hernia repair with high surgical volumes and proven outcomes. At Houston Heartburn and Reflux Center, Dr. Elias Darido focuses exclusively on GERD and hiatal hernia surgery, offering patients extensive expertise and individualized care.
Related Resources
- Nissen Fundoplication: The gold standard anti-reflux procedure, frequently combined with hiatal hernia repair
- Toupet Fundoplication: Learn about the partial wrap alternative
- LINX Procedure: A different surgical approach to treating GERD
- TIF Procedure: An endoscopic approach to treating GERD
- Is GERD Curable?: Understanding your long-term treatment options
- Diet After Fundoplication: What to eat during your recovery
Ready to Find Out If Hiatal Hernia Repair Is Right for You?
Schedule a consultation with Dr. Darido at Houston Heartburn. During your visit, we will review your medical history, discuss your symptoms, and determine whether additional testing or a surgical evaluation is the right next step.
Houston Heartburn serves patients throughout the Greater Houston area, including The Woodlands, Sugar Land, Katy, Pearland, and surrounding communities.
About the Author
Dr. Elias Darido, MD, FACS

Dr. Elias Darido is a board-certified surgeon specializing exclusively in foregut surgery, including acid reflux, hiatal hernia repair, and esophageal conditions. He completed his fellowship in advanced laparoscopic foregut surgery at the University of North Carolina at Chapel Hill and has performed over 1,000 anti-reflux procedures. He is a member of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), the American College of Surgeons (ACS), and the American Society for Metabolic and Bariatric Surgery (ASMBS). Dr. Darido has published numerous peer-reviewed articles on foregut surgery and is a recognized expert in complex and revision anti-reflux surgery.



